Pain Catastrophizing Scale (PCS)⁚ An Overview
The Pain Catastrophizing Scale (PCS) is a widely used self-report measure assessing catastrophic thinking related to pain. It’s a valuable tool in clinical practice and research‚ providing insights into how individuals cope with and perceive pain experiences. The scale’s 13 items assess rumination‚ magnification‚ and helplessness related to pain. Higher scores indicate greater catastrophizing.
The PCS⁚ A Widely Used Assessment Tool
The Pain Catastrophizing Scale (PCS) stands as a prominent self-report instrument employed extensively to evaluate the cognitive and emotional reactions individuals exhibit when confronted with painful sensations. Its widespread adoption stems from its proven reliability and validity across diverse populations‚ making it a valuable tool in both clinical settings and research endeavors. Clinicians utilize the PCS to gauge the extent to which a patient’s thought patterns and feelings amplify their pain experience‚ potentially hindering effective coping strategies and recovery. Researchers frequently incorporate the PCS into studies investigating the relationship between catastrophizing and various pain conditions‚ facilitating a deeper understanding of pain’s psychosocial dimensions. The PCS’s accessibility‚ in the form of readily available PDFs‚ further contributes to its widespread use and influence within the field.
Understanding Pain Catastrophizing
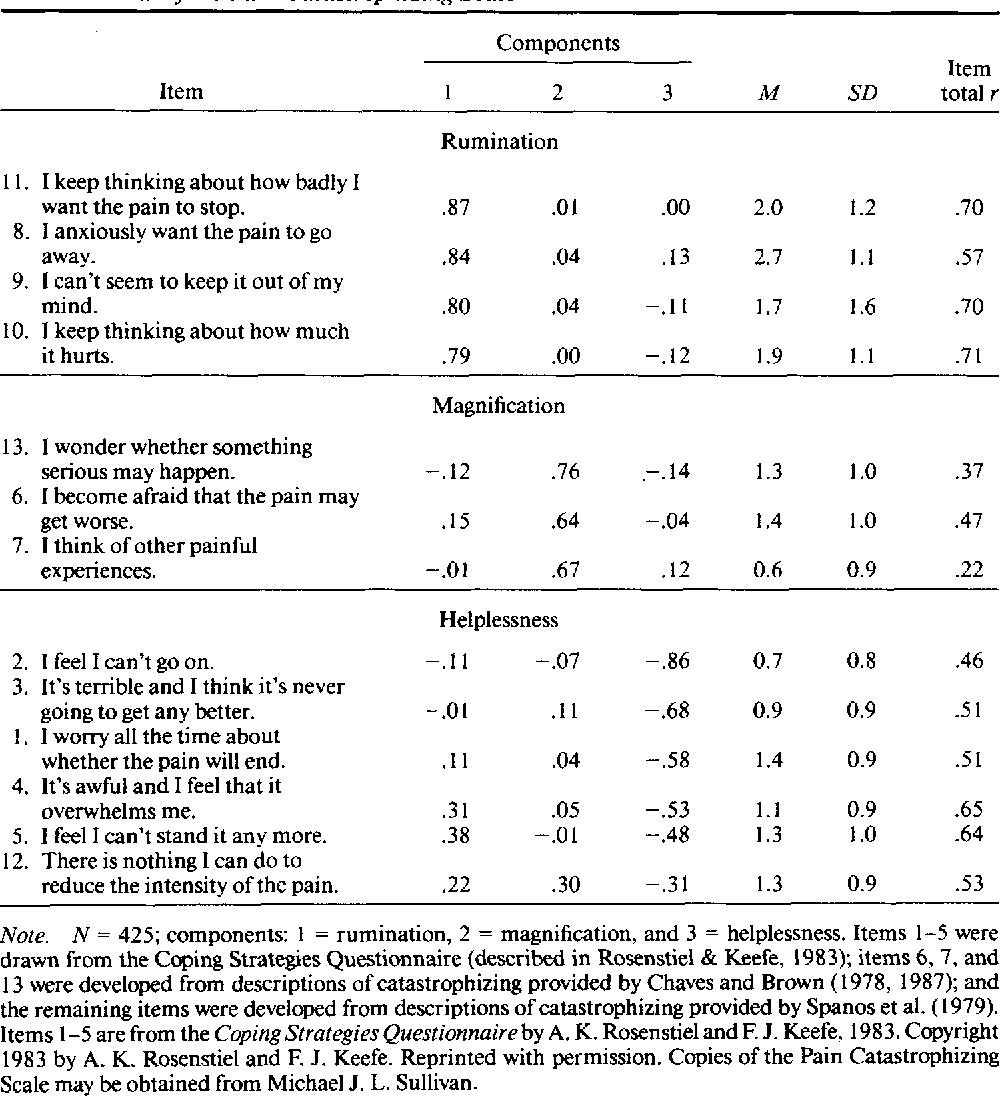
Pain catastrophizing represents a maladaptive cognitive and emotional response to pain‚ significantly impacting an individual’s experience and management of painful sensations. It encompasses three key dimensions⁚ rumination (excessive focus on pain)‚ magnification (overestimating pain’s severity and impact)‚ and helplessness (feeling unable to cope with the pain). Individuals prone to catastrophizing often engage in negative self-talk‚ anticipate the worst possible outcomes‚ and feel overwhelmed by their pain. This negative thought pattern can lead to increased pain perception‚ heightened emotional distress‚ and functional limitations. Understanding these cognitive and emotional components is crucial for developing effective interventions aimed at modifying unhelpful pain-related thoughts and beliefs‚ thereby improving pain management and overall well-being. The PCS helps clinicians identify and quantify the degree of catastrophizing present in their patients.
The Structure and Scoring of the PCS
The Pain Catastrophizing Scale (PCS) is a 13-item self-report questionnaire‚ with each item rated on a 5-point Likert scale (0 = not at all to 4 = all the time). These items assess the three dimensions of pain catastrophizing⁚ rumination‚ magnification‚ and helplessness. Participants indicate how frequently they experience thoughts and feelings related to pain‚ such as worrying excessively about its duration or intensity. The total score ranges from 0 to 52‚ with higher scores indicating a greater tendency towards pain catastrophizing. Clinically significant levels of catastrophizing are often indicated by scores above a certain threshold (e.g.‚ 30)‚ though the specific cut-off may vary depending on the clinical context and population studied. Subscale scores for each dimension provide a more detailed understanding of the patient’s specific pattern of catastrophic thinking. This structured approach allows for both quantitative and qualitative assessment of pain catastrophizing.

Accessing the Pain Catastrophizing Scale PDF
Numerous online resources offer the Pain Catastrophizing Scale (PCS) PDF. Researchers and clinicians can locate the PDF through academic databases‚ professional websites‚ or directly from scale developers. Always verify the source’s legitimacy before using any downloaded version.
Locating Online Resources
Finding a reliable Pain Catastrophizing Scale (PCS) PDF requires careful searching. Begin with reputable academic databases like PubMed or PsycINFO‚ using keywords such as “Pain Catastrophizing Scale‚” “PCS‚” and “questionnaire.” These databases often link to published articles containing the scale as supplementary material or within the study’s methodology section. University websites‚ particularly those of psychology or pain research departments‚ may also host the PCS PDF‚ often within faculty member publications or research project pages. Professional organizations focused on pain management or psychology may provide links to validated versions of the PCS. Exercise caution when encountering PDFs from non-academic sources; always verify the source’s credentials and the scale’s validity to ensure accuracy and ethical use.
Obtaining the PDF Template
Direct access to a freely downloadable PCS PDF template might be limited due to copyright restrictions and the need to ensure proper usage. Many researchers and clinicians obtain the scale through official channels or by contacting the scale’s authors or their designated representatives. Some journals publishing research employing the PCS may provide access to supplementary materials containing the scale. While unofficial versions may appear online‚ using these carries risks⁚ they might be outdated‚ altered‚ or entirely inaccurate. Using an unvalidated version can significantly compromise research integrity or clinical assessment. Therefore‚ seeking the PCS through established academic or professional routes ensures you obtain a legitimate‚ validated version. This ensures the reliability and validity of your results.
Using and Interpreting the PCS
The PCS PDF typically includes clear instructions for administration and scoring. Participants rate 13 statements on a scale (usually 0-4)‚ reflecting their thoughts and feelings during pain experiences. Higher scores indicate greater catastrophizing. The total score ranges from 0 to 52‚ with higher scores suggesting more severe catastrophizing. Additionally‚ the PCS often yields subscales (rumination‚ magnification‚ helplessness)‚ offering a more nuanced understanding of the individual’s response to pain. Interpreting the results requires careful consideration of the context‚ including the individual’s specific pain condition‚ demographics‚ and other relevant factors. Clinicians and researchers often use established cut-off scores to identify individuals who may benefit from targeted interventions. However‚ interpretation should always involve professional judgment.
Applications and Research on the PCS
The PCS is extensively used in clinical settings and research to understand and manage pain. Studies explore its relationship with chronic pain conditions‚ treatment outcomes‚ and various patient populations. It aids in identifying individuals at risk for heightened pain experiences.
Clinical Uses of the PCS
Clinicians utilize the Pain Catastrophizing Scale (PCS) to assess how patients’ thoughts and feelings influence their pain experience. This helps in identifying individuals who may benefit from specific interventions targeting catastrophizing. By understanding a patient’s level of catastrophizing‚ clinicians can tailor treatment plans to address cognitive and emotional factors that contribute to pain perception and management. The PCS assists in guiding treatment choices‚ such as cognitive behavioral therapy (CBT) or other techniques aimed at modifying unhelpful thought patterns and emotional responses to pain. Early identification of high catastrophizing allows for proactive interventions‚ improving treatment outcomes. The PCS also helps monitor treatment progress‚ providing valuable feedback on the effectiveness of interventions designed to reduce pain catastrophizing. Incorporating the PCS into a comprehensive pain assessment contributes to a more holistic and personalized approach to pain management. For example‚ if a patient scores high on the PCS‚ the clinician might recommend CBT to help the patient manage their pain more effectively.
Research Studies Utilizing the PCS
The Pain Catastrophizing Scale (PCS) has been extensively used in research to investigate the role of catastrophizing in various pain conditions. Studies explore the relationship between PCS scores and pain intensity‚ disability‚ and treatment outcomes. Researchers use the PCS to identify factors associated with higher levels of pain catastrophizing‚ such as specific personality traits or coping styles. The PCS is often included in larger studies examining the effectiveness of pain management interventions‚ allowing researchers to determine if interventions targeting catastrophizing improve outcomes. Furthermore‚ the PCS helps researchers understand how catastrophizing interacts with other factors influencing pain‚ like depression or anxiety. Cross-cultural studies using the PCS investigate whether the relationship between catastrophizing and pain varies across different populations. This research informs the development of culturally sensitive interventions to address pain catastrophizing effectively. Longitudinal studies using the PCS track changes in catastrophizing over time‚ helping researchers understand the long-term impact of pain and the effectiveness of chronic pain management strategies.
PCS in Different Populations
The Pain Catastrophizing Scale (PCS) has proven adaptable across diverse populations‚ showcasing its utility in various clinical settings and research contexts. Studies have employed the PCS to assess pain catastrophizing in patients with chronic low back pain‚ fibromyalgia‚ arthritis‚ and other chronic pain conditions‚ revealing significant variations in catastrophizing levels across these groups. The PCS has also been used effectively with pediatric populations‚ although modifications or specialized versions may be necessary to accommodate age-related cognitive and communication differences. Furthermore‚ the PCS has been validated and utilized in research with diverse cultural and linguistic backgrounds‚ highlighting the scale’s robustness and generalizability. Researchers have translated and adapted the PCS for use in various languages‚ extending its application to broader global contexts. However‚ important considerations must be made regarding cultural nuances and potential variations in the interpretation of scale items across different cultural groups. This allows researchers to examine the influence of cultural factors on the experience of pain and catastrophizing behaviors‚ leading to a more comprehensive understanding of how to effectively address pain in different cultural settings.
Further Considerations and Resources
Beyond the PCS‚ other tools assess pain experience. Exploring these alternatives and additional resources can provide a more comprehensive understanding of pain management strategies and research findings.
Limitations of the PCS
While the Pain Catastrophizing Scale (PCS) offers valuable insights into how individuals experience and cope with pain‚ it’s crucial to acknowledge its limitations. The PCS primarily focuses on cognitive and emotional responses to pain‚ neglecting the significant influence of physiological and social factors. Its self-report nature introduces potential biases‚ such as response styles and recall limitations. The scale might not adequately capture the nuances of pain experiences across diverse populations‚ potentially leading to misinterpretations. Furthermore‚ the PCS’s reliance on a single time point might not reflect the dynamic nature of pain and catastrophizing‚ which can fluctuate over time. The three-factor structure‚ while generally supported‚ may not always hold across all patient groups or cultural contexts. Clinicians should consider these limitations when interpreting PCS scores and integrating them into a broader assessment of pain. The PCS should be used in conjunction with other assessment measures for a more comprehensive understanding of the patient’s experience.
Alternative Pain Assessment Tools
Beyond the Pain Catastrophizing Scale (PCS)‚ several other assessment tools provide valuable insights into various aspects of the pain experience. The Pain Beliefs and Perceptions Inventory (PBPI) explores patients’ beliefs about pain and its impact‚ offering a complementary perspective to the PCS’s focus on catastrophizing. The Tampa Scale of Kinesiophobia (TSK) assesses fear of movement‚ a crucial factor in chronic pain conditions. Similarly‚ the Oswestry Disability Index (ODI) specifically focuses on the impact of low back pain on daily activities. For assessing broader psychological distress‚ the Hospital Anxiety and Depression Scale (HADS) can provide valuable information. The choice of alternative tools depends on the specific clinical goals and the nature of the patient’s pain. For instance‚ if fear avoidance is a central issue‚ the TSK might be more appropriate than the PCS. A comprehensive assessment often involves using multiple tools to create a holistic picture of the patient’s pain experience and related psychological factors. Integrating different assessment methods can enhance the accuracy and effectiveness of clinical decision-making.
Additional Resources and Information
For further information on the Pain Catastrophizing Scale (PCS) and related concepts‚ several resources are readily available. The official website of the scale’s developers often provides comprehensive documentation‚ including manuals‚ scoring guidelines‚ and research articles. Academic databases like PubMed and PsycINFO offer a wealth of research articles utilizing the PCS‚ exploring its psychometric properties‚ and examining its relationship with various pain conditions and treatments. Professional organizations such as the American Psychological Association (APA) and the International Association for the Study of Pain (IASP) offer educational materials and resources on pain management and related psychological factors. Textbooks and professional journals dedicated to pain psychology and rehabilitation medicine frequently discuss the PCS and its clinical applications. These resources collectively offer a wealth of information to deepen understanding of pain catastrophizing and its management.
Leave a Reply
You must be logged in to post a comment.